Return to flip book view
Dr WuMengYu talks 2020 Important Concepts in Venovenous ECMO
Kate Meng Yu Wu Kate Wu 1972 2018 KO www drwumengyu com
Hi Kate ECMO Venovenous ECMO workshop3627 gmail com
Concept 1 No more VILI
VV ECMO A R D S
Acute Respiratory Distress Syndrome Thompson BT Chambers RC Liu KD N Engl J Med 2017 Aug 10 377 6 562 572
ARDS ARDS Acute Respiratory Distress Syndrome ARDS 2012 Berlin definition ARDS X CT ARDS 7 PEEP Positive endrespiratory pressure 5
Mortality 45 Who will not survive while treated by MV alone
Berlin definition PF ratio PaO2 FiO2 ARDS 3 PF ratio 100 ARDS 50 50
Mechanical Ventilation is the first respiratory support for ARDS
The Principle of MV Open the Lung and Keep it Open Trans lung pressure No PEEP PEEP 12
1 open the lung and keep it open translung pressure PEEP translung pressure PEEP PEEP
PEEP ARDS dp dt PEEP 25 P1 50 P2 25 50 P2 P1 VP P2 P1 P1 PEEP
Open the Lung Need a warm up C dV dP Px P1 P2 15 Berne Levy Physiology 6th ed P434 P3
PEEP VP PX PEEP PX
2 peak inspiratory pressure PIP plateau pressure Pplt
MV driving pressure Ppt PEEP
pressure control mode PIP Pplt Pplt 30 Driving pressure Pplt PEEP Tidal volume VT driving pressure Compliance
driving pressure ARDS driving pressure driving pressure 13
VQ Mismatch 1 driving pressure FiO2 A R D S dependent part
Inhomogeneous Aerated Lung in ARDS VILI enhances V Q mismatch Dependent lower lobes Absorptive atelectasis Independent upper lobes Over Aerated 22
Ventilation V Perfusion P VQ match Q Perfusion
VQ Mismatch 2 ARDS 3 VQ mismatch dead space ventilation shunting
Dead space Ventilation Mosaic area Atelectasis 26 V Q Better VQ match V
ARDS VQ mismatch diastolic failure
Rationale of ARDS Deteriorating on MV Hypoxemia Hypotension Acute Cor Pulmonale AKI
VQ Mismatch ARDS FiO2 VQ mismatch
Lung Protective Ventilation Low tidal volume and higher PEEP
1 VQ Mismatch VQ mismatch Dead space ventilation VT Lung Protective ventilation LPV
The Rationale of LPV Dead space ventilation LPV recruited Conventional MVrecruited Shunting
2 LPV Baby lung driving pressure CT baby lung LPV VQ mismatch VT VQ mismatch
Extracorporeal membrane oxygenation ECMO
PF ratio 70
CGMH Linko VVECMO Protocol All cause
Concept 2 Competing pumps
vs
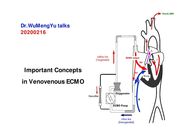
Venovenous ECMO Q0 venous blood Q1 ECMO oxygenated blood recirculated Q2 ECMO oxygenated blood not recirculated Q3 Mixed blood partially refreshed by ECMO Q4 Pulmonary oxygenated blood Arterial blood Q4 is the key for the speed to downgrade the setting of MV
VVECMO ECMO Pump pump ECMO pump Q3 Q3 VVECMO Q3 LPV
RA PA Ao The lungs still need to be Functional
Baby lung Q3 Q4 FiO2 FiO2
FiO2 ARDS driving pressure
Adjust Pump Flow Pumps Competition 3 2
VVECMO VVECMO PIP ECMO gas flow 1
PICCO ECMO pump flow ECMO pump ECMO PICCO pump flow Spo2 pump flow Spo2 PICCO 2 4 PRBC pump flow
Adjust Gas Flow Crosstalk between MV and ECMO 3 2 Reduce VILI Pressure first SPo2 90
ECMO Gas Flow Gas flow ECMO FiO2 100 FiO2 VVECMO LPV PIP 30 cmH2O PEEP 12 14 cm H2O FiO2 40 SaO2 90 PaO2 70mmHg PaCO2 30 40 mmHg
Factors Determining ECMO Gas Exchange Gas flow More CO2 washed out than Oxygenation in ECMO
10 gm dL ECMO CRRT ECMO CRRT ECMO CRRT CRRT
Recirculation ECMO flow recirculation ECMO 15 SVC
Venovenous Mode Prepulmonary Gas Exchange to Reduce VILI Mode for ARDS without shock
RV ECMO
VA VVA ECMO FiO2 PIP 30 cmH2O PEEP 12 14 cmH2O FiO2 60 40
Concept 3 Coagulopathy
Modest Anti coagulation aPTT 45 60 seconds
An Extreme Hypocoagulation This hypocoagulation state was reversed after 12 hours in patients without or with a mild TIC Wu MY et al Venovenous extracorporeal life support for posttraumatic respiratory distress syndrome in adults the risk of major hemorrhages Scand J Trauma Resusc Emerg Med 2014 Oct 2 22 56
2000 5000 aPTT aPTT 6 8 aPTT 40 50 aPTT 40 50 Protamine
Concept 4 Dry Lungs
Lung Water
Daily I O 63
I O negative volume control bolus ECMO blood flow ECMO blood flow
Concept 5 A Protocol
protocol
QR code
ARDS ARDS
ARDS 10 14 compliance PF ratio VQ mismatch PF ratio 70 200 baby lung ARDS
Increased pre ECMO MV duration Increased consumption of pulmonary compliance Increased driving pressure on respiratory support Increased hospital mortality rate after respiratory ECMO Survivors presentation
Take a rest but not in the end