Return to flip book view
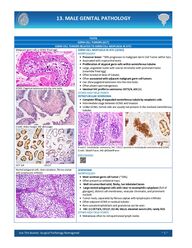
Ace The Boards: Surgical Pathology Reimagined ~ 1 ~ 13. MALE GENITAL PATHOLOGY TESTIS GERM CELL TUMORS (GCT) GERM CELL TUMORS RELATED TO GERM CELL NEOPLASIA IN SITU Malignant germ cells in GCNIS (fried egg) GCNIS: Pagetoid extension into the rete testis Credit: Ankur Sangoi, MD @slusagar OCT 3/4 CD117 GERM CELL NEOPLASIA IN SITU (GCNIS) MORPHOLOGY • Precursor lesion: ~50% progresses to malignant Germ Cell Tumor within 5yrs. • Associated with cryptorchid testis • Proliferation of atypical germ cells within seminiferous tubules • Large, angulated nuclei with coarse chromatin with prominent halos (resemble fried egg) • Often located at base of tubules • Often associated with adjacent malignant germ cell tumors. • Can show pagetoid extension into the rete testis • Often absent spermatogenesis. • Identical IHC profile to seminoma: OCT3/4, cKit (+) OTHER HIGH YIELD POINTS INTRATUBULAR SEMINOMA • Complete filling of expanded seminiferous tubule by neoplastic cells • Intermediate stage between GCNIS and Invasion • Unlike GCNIS, Sertoli cells are usually not present in the involved seminiferous tubules H and E: intratubular seminoma, IHC: CD117 positive in intratubular seminoma and GCNIS Credit: Gladell Paner, MD @GladellPaner Path Presenter Nested polygonal cells, clear cytoplasm, fibrous septae with lymphocytic infiltrate SEMINOMA MORPHOLOGY • Most common germ cell tumor (~50%). • Often present as unilateral mass. • Well circumscribed solid, fleshy, tan lobulated lesion • Large nested polygonal cells with clear to eosinophilic cytoplasm (full of glycogen), distinct cell membranes, vesicular chromatin, and prominent nucleoli • Tumor nests, separated by fibrous septae with lymphocytic infiltrate • Often adjacent GCNIS in residual tubules • Rare syncytiotrophoblasts and granuloma can be seen • IHC: (+) OCT3/4, CD117, D2-40, SALL4, elevated serum LDH, rarely hCG OTHER HIGH YIELD POINTS • Metastases often to retroperitoneal lymph nodes
Ace The Boards: Surgical Pathology Reimagined ~ 2 ~ 13. MALE GENITAL PATHOLOGY Striped/ Tigroid appearance on smear in Seminoma Granuloma often seen Rarely Signet ring-like cell can be seen Seminoma gross appearance; Credit: Wikimedia Commons Path Presenter • Molecular: majority have isochromosome 12p; c-kit mutations • Prognosis: Good if treated, chemo sensitive OCT 3/4 Positive CD117 Positive Seminoma IHC (credit: Beatriz Agredano, MD, Spain)
Ace The Boards: Surgical Pathology Reimagined ~ 3 ~ 13. MALE GENITAL PATHOLOGY Embryonal carcinoma Necrosis Prominent nucleoli, mitosis, apoptosis EMBRYONAL CARCINOMA MORPHOLOGY • Second-most common testicular GCT, usually part of a mixed GCT • Composed of rudimentary cells with epithelial differentiation and marked cytologic atypia • Variety of growth patterns (nests, sheets, papillae, glands) • Large, crowded, “Primitive” pleomorphic cells with vesicular nuclei, basophilic chromatin, prominent nucleoli and amphophilic cytoplasm • Prominent mitoses and apoptotic bodies are present • Frequent hemorrhage and tumor necrosis • Intratubular EC with comedonecrosis and coarse calcification • IHC: Positive for CD30, OCT3/4, AE1/AE3, SALL4 OTHER HIGH YIELD POINTS • Molecular: Isochromosome 12p amplification • Prognosis: Aggressive, but often responds to chemotherapy Embryonal carcinoma IHC (credit: Beatriz Agredano, MD, Spain) Variegated appearance with hemorrhage and necrosis OCT 3/4
Ace The Boards: Surgical Pathology Reimagined ~ 4 ~ 13. MALE GENITAL PATHOLOGY INTRATUBULAR EMBRYONAL CARCINOMA (ITEC) • Complete filling of expanded seminiferous tubule by neoplastic cells • Precursor lesion of non - seminomatous tumor Figure: Intratubular Embryonal carcinoma with adjacent GCNIS Credit: Gladell Paner, MD Path Presenter Extensive hemorrhage and necrosis Viable tumor at the periphery Lymphovascular invasion CHORIOCARCINOMA MORPHOLOGY • Usually, a part of a mixed GCT • Extensive hemorrhage and necrosis with little viable tumor at the periphery • Tumor is composed of mixture of Syncytiotrophoblasts giant cells and mononuclear trophoblastic cells (cytotrophoblasts) and intermediate trophoblasts. • Lymphovascular invasion and blood vessel invasion is very common • STGC have numerous hyperchromatic nuclei and abundant cytoplasm with distinct cytoplasmic vacuoles • Smaller cells are the cytotrophoblasts and intermediate trophoblastic cells with distinct cell borders, pale cytoplasm, mildly pleomorphic nuclei, and prominent nucleoli, they form tight clusters • IHC: Positive hCG, Syncytiotrophoblasts: Positive for inhibin, glypican-3 • Cytotrophoblasts: Positive for SALL4, p63, GATA3 • Elevated Serum hCG OTHER HIGH YIELD POINTS • Most aggressive GCT, less responsive to treatment • Frequent early hemorrhagic metastases to lung OCT 3/4, B-HCG, GATA3 and Glypican stains. Path presenter
Ace The Boards: Surgical Pathology Reimagined ~ 5 ~ 13. MALE GENITAL PATHOLOGY Yolk Sac tumor Schiller-Duval Bodies Hyaline globules Path Presenter YOLK SAC TUMOR, POSTPUBERTAL-TYPE/ ENDODERMAL SINUS TUMOR MORPHOLOGY • Almost always a component of mixed GCT • Many patterns/architecture (often combined) • Growth patterns recapitulate yolk sac, allantois, and extraembryonic mesenchyme • Most common pattern reticular/microcystic (Honeycomb meshwork) • Can also be solid, papillary, glandular, etc • Often hypocellular myxoid areas are present • Schiller-Duval Bodies, refractile eosinophilic hyaline globules and band-like intercellular basement membrane material are helpful clues • IHC: Positive for AFP, Glypican-3, SALL4, AE1/AE3 OTHER HIGH YIELD POINTS • Elevated Serum AFP • Common in Post-chemo cases (sarcomatoid YST) • Can have “hepatoid” areas resembling liver that stains with liver markers OCT3/4 Glypican AFP Teratoma Rhabdomyosarcoma in a teratoma Credit: Andres Martin Acosta MD @Andres_M_Acosta TERATOMA, PREPUBERTAL-TYPE MORPHOLOGY • Most common component in a treated GCT • Composed of tissues from one or more germinal layers • May be composed of mature and /or immature, embryonic-type tissue • Often part of a mixed GCT • Composed of multiple cysts lined by glandular or squamous epithelium • Often areas of cytologic atypia, including primitive mitotically active stroma cuffing glands are present • Frequent immature neuroectodermal structures can be seen SOMATIC-TYPE MALIGNANCY ARISING IN A TERATOMA • If a dysplastic component forms a nodule that is larger than a 4X field (5 mm) • Usually a sarcoma, most commonly rhabdomyosarcoma • Most common carcinoma is adenocarcinoma of various growth patterns OTHER HIGH YIELD POINTS • Unlike ovary, all teratomas in post pubertal testis are malignant! • Rare situation benign teratoma can occur in an adult: Dermoid cysts, or prominent components of ciliated epithelium and smooth muscle • However, no GCNIS, isochrome 12p, or testicular scarring should be noted Path Presenter
Ace The Boards: Surgical Pathology Reimagined ~ 6 ~ 13. MALE GENITAL PATHOLOGY GERM CELL TUMORS UNRELATED TO GERM CELL NEOPLASIA IN SITU Spermatocytic tumor (3 cell types: small, medium & large) Credit: Andres Martin Acosta MD Credit: Phoenix Bell MD @PhoenixBellMD SPERMATOCYTIC TUMOR MORPHOLOGY • Relatively rare • Usually occurs in older men (>50yo) • NOT associated with GCNIS or cryptorchidism • Polymorphous cell population (3 cell types: small, medium, and large) • Tumor cells with poorly defined cell membranes, dense cytoplasm, • Round nuclei with dense to granular chromatin • Diffuse to multinodular pattern of growth. • Frequent cystic change/edema are present • No significant inflammation/granulomas are seen • IHC: Negative for usual seminoma markers, + SALL 4, CD117 (50%), SSX • Can undergo sarcomatous transformation OTHER HIGH YIELD POINTS • Excellent prognosis • NOT a component of mixed GCT SSX D2-40 SALL4 OCT3/4 CD117 Teratoma Epidermoid cyst TERATOMA, PREPUBERTAL-TYPE MORPHOLOGY • Composed of tissues from one or more germ cell layers • Primarily occurs in prepubertal males <6 years old • Frequently include skin structures, ciliated epithelium, fat, cartilage, bone, and muscle in organoid structures SPECIALIZED VARIANTS: • Dermoid Cyst: replicate skin • Squamous epithelium with adnexal structures • Epidermoid Cyst: Unilocular cyst with squamous lining and keratinaceous debris. No adnexal structures or other elements • Well-differentiated Neuroendocrine Tumor: Similar morphology to elsewhere. Often pure. Usually good behavior, can behave aggressively OTHER HIGH YIELD POINTS • Unlike Post pubertal type: Benign behavior, do not recur or metastasize • NO association with GCNIS, tubular atrophy, scar or isochrome 12p amplification • NO association with mixed GCT • Like mature cystic teratomas seen in the ovary
Ace The Boards: Surgical Pathology Reimagined ~ 7 ~ 13. MALE GENITAL PATHOLOGY YOLK SAC TUMOR, PREPUBERTAL-TYPE MORPHOLOGY • Identical morphology and IHC profile to post pubertal type • Secretes AFP OTHER HIGH YIELD POINTS • Rare • Usually in young boys <6 years old • Usually pure, but can see in combination • Unlike post pubertal YST: NOT associated with GCNIS or isochrome 12p amplification • Excellent survival, even with advanced stage Regressed Seminoma REGRESSED GERM CELL TUMORS MORPHOLOGY • Well-delineated nodular focus of scaring fibrosis in the testis • Germ cell tumors that have undergone either partial or complete regression (“burnt-out”) • Can present with metastatic disease, even after complete regression of primary tumor • Can be seminoma or non-seminomatous. • Coarse calcifications within tubules, chronic inflammation, hyalinized tubular ghosts cells can be seen • GCNIS, tubular atrophy, microliths may also seen Path Presenter Mixed Germ Cell Tumor MIXED GERM CELL TUMOR MORPHOLOGY • Malignant tumors with more than one germ cell tumor component • Clinically regarded as “non-seminoma” (even if seminoma present) • Majority of all non-seminomatous GCT are mixed • Must report approximate % of each component OTHER HIGH YIELD POINTS • Syncytiotrophoblasts ≠ choriocarcinoma (can see in other tumors, like seminoma) SPECIAL SUBTYPES: • Polyembryoma: Embryonal carcinoma and YST resembling an embryo • Diffuse embryoma: Embryonal carcinoma and YST in parallel flat layers Diffuse embryoma