Return to flip book view
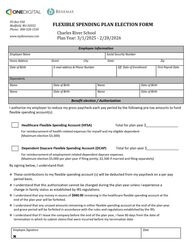
PO Box 950Medfield, MA 02052Phone: 800-528-1530www.myBenemax.comFLEXIBLE SPENDING PLAN ELECTION FORMCharles River SchoolPlan Year: 3/1/2025 - 2/28/2026By signing below, I understand that:❖ These contributions to my flexible spending account (s) will be deducted from my paycheck on a per pay period basis. ❖ I understand that this authorization cannot be changed during the plan year unless I experience a change in family status as established by IRS regulations. ❖ I understand that any money in excess of $660.00 remaining in the healthcare flexible spending account at the end of the plan year will be forfeited.❖ I understand that any unused amounts remaining in either flexible spending account at the end of the plan year and grace period will be forfeited in accordance with the rules and regulations established by the IRS. ❖ I understand that if I leave the company before the end of the plan year, I have 90 days from the date of termination in which to submit claims that were incurred before my termination date.Employee SignatureXDateEmployee InformationEmployee NameSocial Security NumberHome Address Street City State ZipDate of BirthE-mail address & Phone NumberEff. Date of EnrollmentFirst Payroll DateDependentsNameDate of BirthNameDate of BirthNameDate of BirthNameDate of BirthBenefit election / AuthorizationI authorize my employer to reduce my gross paycheck each pay period by the following pre-tax amounts to fund flexible spending account(s): Healthcare Flexible Spending Account (HFSA) Total for plan year $_________________For reimbursement of health-related expenses for myself and my eligible dependent (Maximum election $3,300)Dependent Daycare Flexible Spending Account (DCAP) Total for plan year $_________________For reimbursement of employment related dependent daycare expenses (Maximum election $5,000 per plan year if filing jointly; $2,500 if married and filing separately)